De Quervain's Tenosynovitis
What is De Quervain's Tenosynovitis?
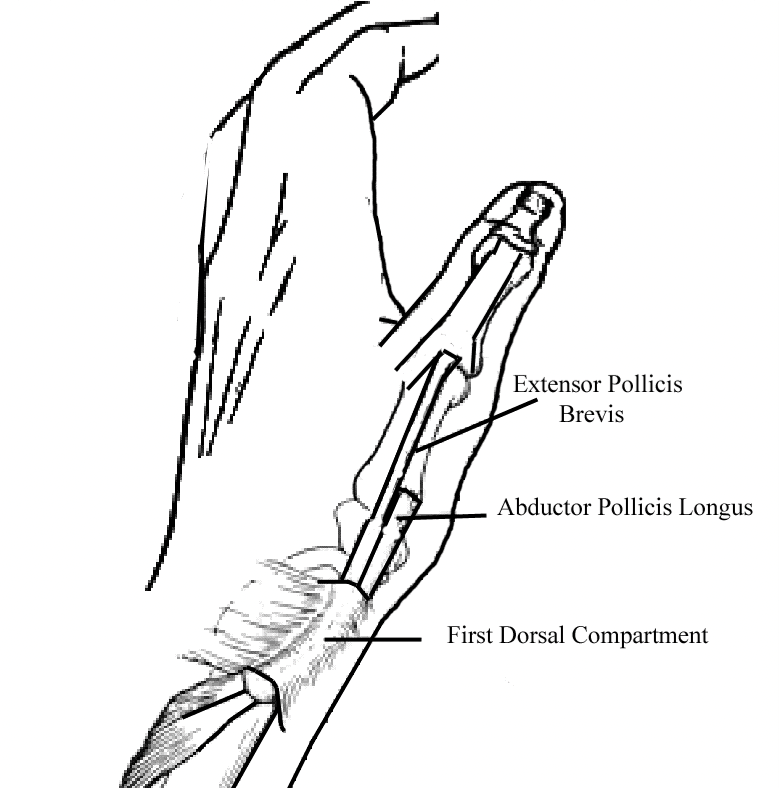
De Quervain’s Tenosynovitis is a painful irritation of the tendons on the thumb side of the wrist. A Swiss surgeon, Fritz de Quervain, described the problem in 1895. Passing over the back (or dorsal surface) of the wrist are the tendons that straighten the thumb, fingers, and wrist. These tendons run through six tunnels (compartments) under a thick fibrous layer called the extensor retinaculum.
De Quervain’s tenosynovitis affects the tendons of the first dorsal compartment. The lubricating sheath lining this tunnel thickens and swells, giving the enclosed tendons less room to move. Fine fibres of scar (adhesions) may form between the lining sheath and the tendons.
What are the causes?
The tendon irritation may be caused by anything that causes swelling or thickening of the tendons. Overuse, particularly in parents caring for infants, and inflammatory processes are all common causes but frequently the cause is unknown.
Who is likely to develop this problem?
• People between 30 and 50 years of age.
• 10 times more common in women.
• Mothers with young infants due to a combination of overuse and hormone-related tendon swelling.
• Repetitive activities can precipitate the symptoms.
• Inflammatory conditions such as rheumatoid arthritis that cause tendon swelling.

What are the signs & symptoms?
The main symptom is pain over the thumb side of the wrist. It may develop suddenly or gradually. It is worse with use of the hand and thumb, especially with forced grasping, pinching, and twisting. There may be swelling at the site of pain and “snapping” when the thumb is moved. Due to pain and swelling, thumb movement may be reduced.
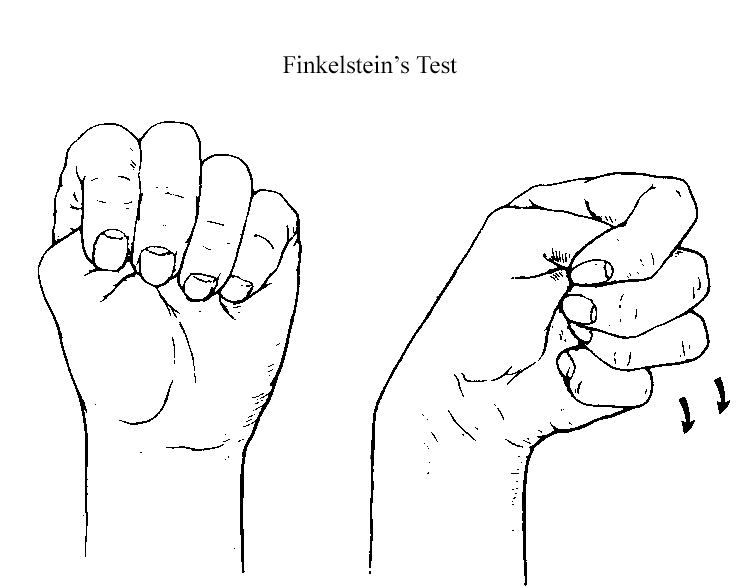
A positive Finkelstein’s test is usually present. In this test, the patient makes a fist with the thumb placed in the palm and bends the wrist. This test will cause pain in patients with de Quervain’s tenosynovitis.

How is it treated?
Non-operative treatment
The initial treatment is to rest the wrist in a splint that immobilizes the wrist and thumb for 4 weeks. A steroid injection into the tendon sheath is usually recommended as this is a strong anti- inflammatory that helps reduce the tendon swelling. The splint is worn day and night and is only taken off to shower or wash the hand. After four weeks in a splint, the hand therapist will start a series of stretching exercises to regain movement. If the symptoms are longstanding (more than 3 months) or the non-operative treatment with a splint and steroid injection has failed, surgery is indicated.
When is surgery necessary?
If the symptoms are longstanding (more than 3 months) or the non-operative treatment with a splint and steroid injection has failed, surgery is indicated.
Surgical treatment
The first dorsal compartment release is a small operation and can performed under general anaesthetic or local anaesthetic and sedation. A 1-2 cm incision is made in a skin crease at the wrist and the first compartment is divided so that there is more room for the tendons to glide with movement.
Risks
Recurrence of the symptoms is very rare. The surgery is safe and very reliable. There is a very small risk of injury to the small nerves resulting in a numb patch on the back of the thumb. Very rarely the tendons can become unstable and require a second surgery.
What about recovery?
Day of surgery: A dressing including a lightweight fibreglass splint is applied at the time of surgery.
2 days: Pain relief may be required, and the hand should be kept elevated to chest height.
2 weeks: Dressings & splint removed, and an exercise program is started. Recommence driving.
2 months: Completing all light daily activities with minimal discomfort.
3-4 months: Returned to normal activities without discomfort. All swelling resolved.