
 Carpal tunnel release is performed as a day surgery procedure under sedation with local anaesthetic or general anaesthetic. The procedure takes approximately 45 minutes. Expect to arrive at the hospital 2 hours before surgery and leave the hospital 2 hours after the surgery. The carpal tunnel release is performed through a 2.5cm skin incision at the base of the palm.
Carpal tunnel release is performed as a day surgery procedure under sedation with local anaesthetic or general anaesthetic. The procedure takes approximately 45 minutes. Expect to arrive at the hospital 2 hours before surgery and leave the hospital 2 hours after the surgery. The carpal tunnel release is performed through a 2.5cm skin incision at the base of the palm.
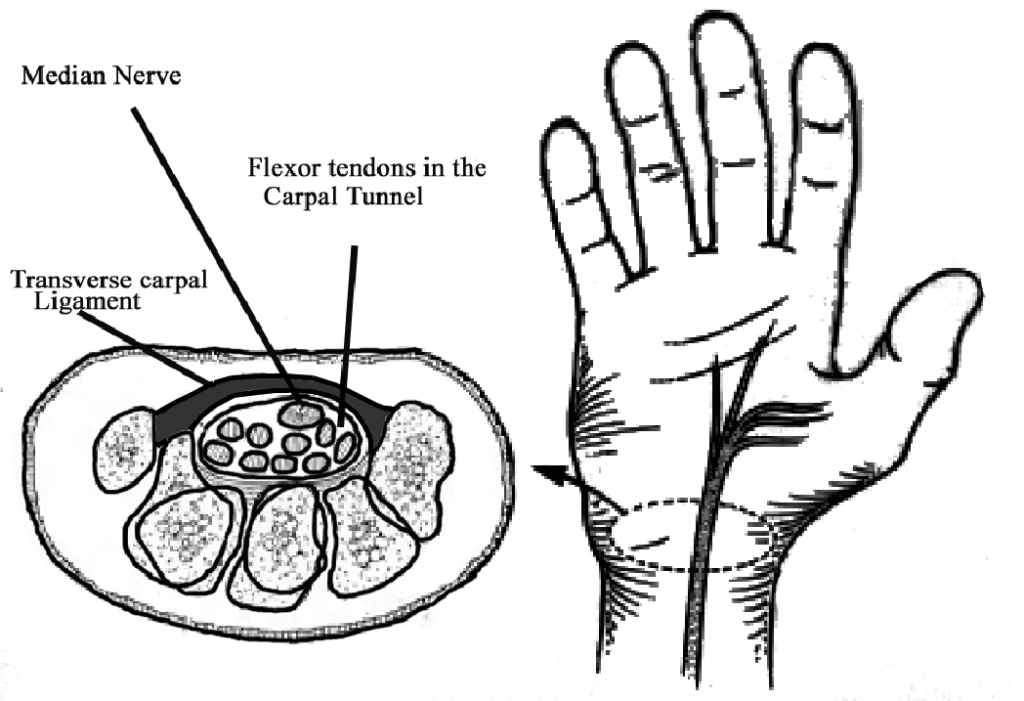
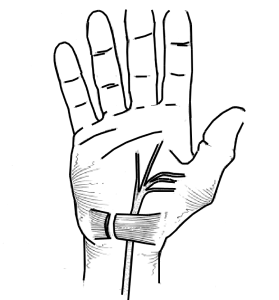
The ligament forming the roof of the tunnel is cut. This allows the tunnel to expand increasing the size of the tunnel by 20% to relieve the pressure on the median nerve. Dissolving stitches are used (unless you are diabetic) and a bandage
is wrapped around the palm and wrist. It is possible to use the fingers and thumb for light activities on the day of surgery. A long-acting local anaesthetic is injected which will make your hand numb for at least 6-8 hours.